The Changing Landscape of Heart Failure Care
Heart failure (HF) continues to be a major public health challenge, affecting more than 6 million adults in the United States alone. Despite advances in therapy, hospitalizations and mortality remain high—often because patients do not receive the full spectrum of evidence-based care.
Over the past few years, major updates from the AHA/ACC/HFSA guidelines (most recently updated in 2022) have transformed how we diagnose, stratify, and manage both heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF).
These updates represent not just incremental change but a fundamental paradigm shift—one that all clinicians managing cardiovascular or chronic disease should understand and apply.
Four Foundational Pillars of HFrEF Therapy
The new standard of care for patients with HFrEF now centers on four medication classes, each supported by robust clinical trial evidence showing reduced mortality and hospitalization.
- ARNI (Angiotensin Receptor–Neprilysin Inhibitor)
- Sacubitril/valsartan is now the preferred first-line agent, shown to reduce death and heart failure hospitalization compared with ACE inhibitors or ARBs in Stage C and D Class II-IV patients with both HFpEF and HFrEF.
- When ARNI cannot be used, an ACE inhibitor or ARB remains an acceptable alternative.
- Evidence-Based Beta-Blocker
- Carvedilol, metoprolol succinate, or bisoprolol improve survival and should be used in all patients unless contraindicated.
- Mineralocorticoid Receptor Antagonist (MRA)
- Spironolactone or eplerenone improve outcomes, particularly among patients with HFrEF NYHA class II–IV symptoms and adequate renal function.
- SGLT2 Inhibitor (Empagliflozin or Dapagliflozin)
- Initially developed for diabetes, these agents have demonstrated substantial benefits in both diabetic and non-diabetic patients with HFrEF and HFpEF, lowering hospitalization and cardiovascular mortality.
Importantly, the guidelines now emphasize that these therapies should be initiated rapidly and in combination, rather than sequentially over months. Evidence shows that early comprehensive therapy dramatically improves outcomes—even within a few months.
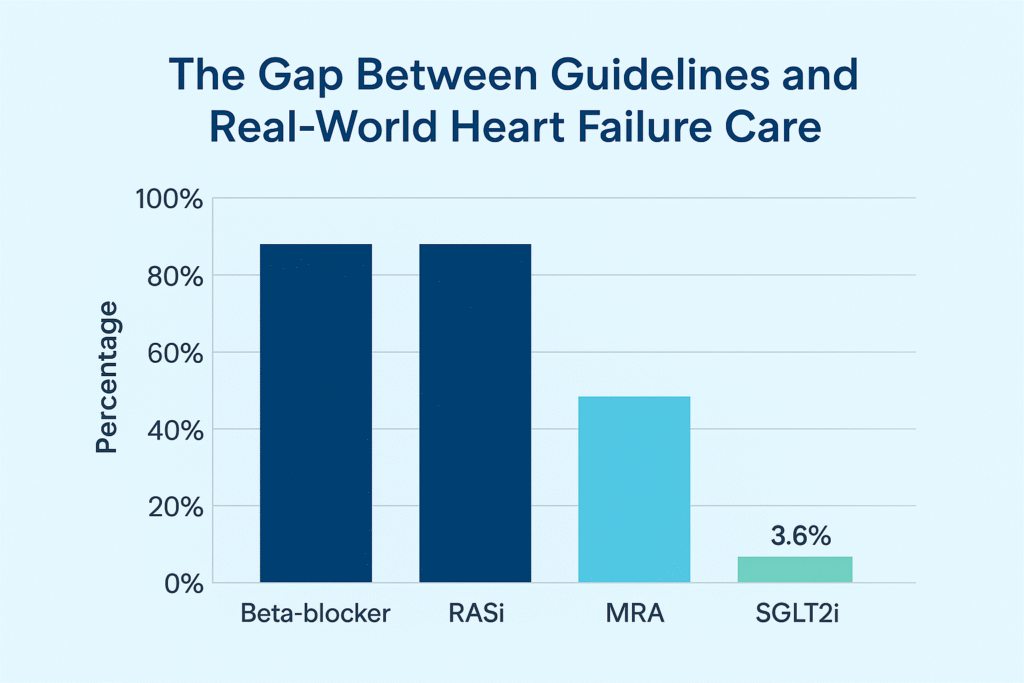
The Gap Between Guidelines and Real-World Heart Failure Care
Despite strong guideline recommendations for quadruple therapy in heart failure with reduced ejection fraction—consisting of a beta-blocker, renin-angiotensin system inhibitor (RASi), mineralocorticoid receptor antagonist (MRA), and sodium-glucose cotransporter 2 inhibitor (SGLT2i)—real-world adoption remains far from optimal. While beta-blocker and RASi use approaches 80%, MRA use drops to about 41%, and SGLT2i therapy lags dramatically at under 4%. This striking gap highlights the persistent challenge of translating evidence-based recommendations into clinical practice, underscoring the need for better education, system-level support, and follow-up to ensure patients receive the full mortality and morbidity benefits of guideline-directed therapy.
Heart Failure with Preserved Ejection Fraction (HFpEF): Finally, Evidence of Progress
For decades, HFpEF has frustrated clinicians due to the lack of effective therapy. That has finally changed.
Recent trials such as EMPEROR-Preserved and DELIVER demonstrated that SGLT2 inhibitors significantly reduce hospitalization in patients with HFpEF, earning them a Class IIa recommendation in the guidelines. Similarly, ARNIs and MRAs now have a Class 2B indication in selected patients with HFpEF to reduce hospitalizations.
Additional strategies include:
- Rigorous blood pressure control
- Management of atrial fibrillation
- Use of MRAs in selected patients
- Aggressive treatment of comorbidities such as obesity, diabetes, and CKD
Together, these represent the most promising therapeutic landscape HFpEF has ever seen.
Beyond Medications: A Holistic Approach
The guidelines now stress a multidisciplinary model of care, integrating:
- Patient education and medication adherence support
- Remote monitoring for early detection of decompensation
- Team-based management, including nurses, pharmacists, and primary care providers
- Lifestyle modification—particularly sodium restriction, physical activity, and weight management
Effective heart failure care is no longer the domain of cardiologists alone; it’s a shared responsibility across the care continuum.
Why Many Patients Still Don’t Receive Guideline-Directed Therapy
Despite overwhelming evidence, real-world implementation lags behind. Studies show that fewer than half of eligible patients receive all four guideline-directed therapies.
Common barriers include:
- Therapeutic inertia or hesitancy to adjust medications quickly
- Concerns about polypharmacy and side effects
- Lack of familiarity with the updated recommendations
- Fragmentation of care and limited follow-up
This is where continuing medical education (CME) can have a transformative impact—if designed effectively.
Reimagining CME: From Information to Implementation
Traditional CME often fails to create sustained change. Clinicians attend a lecture, feel inspired, and then return to their busy practice without structured follow-up.
At CME Travel Academy, we believe learning should mirror how memory actually works.
Our approach combines:
- Live CME sessions (both online and at destination conferences)
- A one-page point-of-care reference for quick clinical decision support
- Twelve months of spaced-repetition follow-up, ensuring retention and real-world application
This model bridges the gap between knowledge and action—helping clinicians implement guideline-directed therapy confidently and consistently.
Join Us: Learn, Relax, and Recharge
CME Travel Academy offers engaging CME experiences in beautiful destinations—because great learning happens when the mind is refreshed.
Upcoming events include:
- New Orleans CME Conference in March 2026 – Focus on Top Chronic Conditions in America including CHF
- Las Vegas CME Conference in March 2026 – Focus on chronic disease management
- San Diego CME Conference in May 2026 – Featuring updates in cardiovascular and metabolic medicine
- Caribbean CME Cruise (coming soon) – A one-of-a-kind blend of education, networking, and relaxation at sea
- Disney World CME Conference in July 2026 – enjoy Disney and learn the latest updates!
Each course includes the same evidence-based foundation and long-term spaced-repetition curriculum designed to make learning stick.
Take the next step toward mastering the latest in heart failure management—and rediscover why you love practicing medicine.
Learn more and see all our upcoming 2026 conferences.
Key Takeaways
- The latest heart failure guidelines establish four foundational medication classes: ARNI, beta-blocker, MRA, and SGLT2 inhibitor.
- SGLT2 inhibitors now play a central role in both HFrEF and HFpEF.
- Early combination therapy is superior to stepwise titration.
- Holistic care, multidisciplinary support, and patient engagement are essential.
- CME that uses spaced repetition and 1-page point-of-care reminders can help translate evidence into daily practice.