A Missed Opportunity: SGLT2 inhibitors in Heart Failure Care
Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have transformed heart failure management, reducing both hospitalizations and cardiovascular deaths across the ejection fraction spectrum. Guidelines now recommend SGLT2i as foundational therapy for patients with heart failure—yet real-world prescribing still lags far behind.
A new retrospective cohort study of over 759,000 patients in the NCDR PINNACLE registry—a national registry of U.S. cardiology practices—found that fewer than 1 in 6 patients with heart failure received an SGLT2 inhibitor from 2019 to 2023.
That’s right: even in specialist cardiology clinics, where awareness of the evidence should be highest, the majority of patients who stood to benefit from these therapies never received them.
What the Study Showed: Low Utilization of SGLT2 inhibitors in Heart Failure
- Low baseline adoption: Only 4.6% of heart failure patients were prescribed SGLT2i in 2019. By 2023, this rose to 16.2%—better, but still leaving most patients untreated.
- Differences by EF: Use was higher in HFrEF (28.5%) than in HFmrEF/HFpEF (12.8%), despite proven benefits across EF categories.
- Disparities in care: Older patients, women, and those with higher systolic blood pressure were less likely to be prescribed therapy. Diabetes remained the strongest predictor of use.
- Practice-level gaps: Even after adjusting for patient factors, there was a fourfold difference in prescribing rates between cardiology practices.
Why This Matters for Clinical Practice
If uptake is this low among cardiologists, it underscores how wide the treatment gap is likely to be in primary care, where many heart failure patients are managed day-to-day.
This means:
- Guidelines aren’t enough—implementation requires system-level strategies.
- Disparities persist—older adults and women are being left behind.
- Primary care adoption is critical—because that’s where most patients are seen and treated long-term.
CME Travel Academy’s Role
At CME Travel Academy, we recognize that closing this gap requires more than knowing the science. It requires practical tools, ongoing reinforcement, and a system-wide approach.
That’s why our programs emphasize:
- Hands-on CME sessions to help clinicians—cardiologists and primary care providers alike—confidently prescribe SGLT2i.
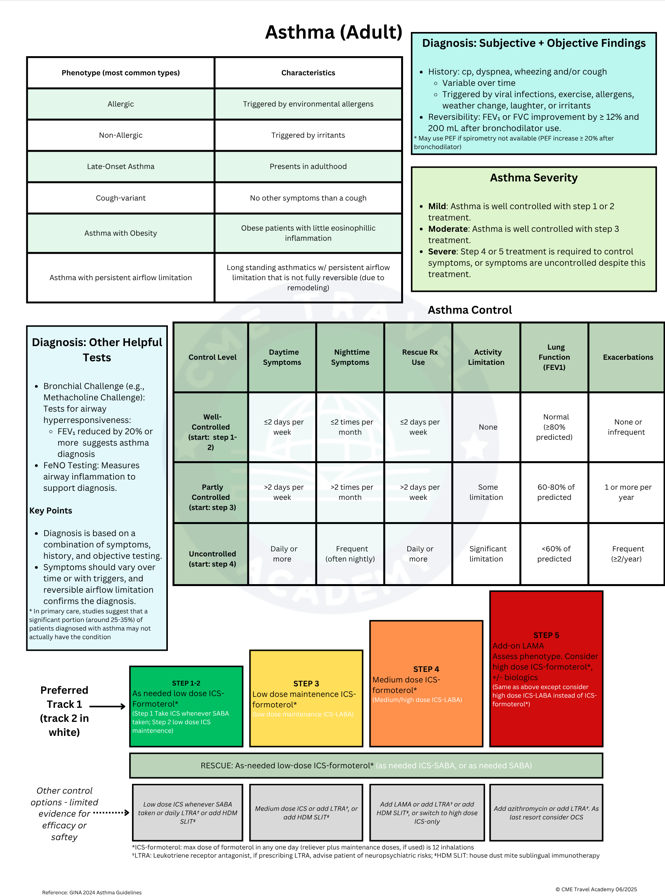
- One-page reference guides (see sample) for point-of-care decision-making.
- 12-month spaced repetition follow-up to keep the evidence fresh and actionable long after the course ends.
{kind=link}
Our mission is simple: ensure that the life-saving benefits of SGLT2 inhibitors are not just known, but applied consistently across both specialty and primary care settings.
Bottom line: If SGLT2 inhibitor use is low even among cardiologists, the challenge in primary care is even greater. CME Travel Academy equips clinicians to close this gap so that every patient with heart failure has access to the therapies proven to improve survival.