Chronic Obstructive Pulmonary Disease (COPD) remains a leading cause of morbidity and mortality worldwide. The 2025 COPD Guidelines bring forward significant updates designed to improve early recognition, personalize treatment, and prevent exacerbations. These changes reflect both evolving evidence and the growing recognition that COPD is not a “one-size-fits-all” condition, but a complex disease with heterogeneous presentations.
For clinicians in primary care, family medicine, internal medicine, and pulmonary specialties, the 2025 updates provide essential tools for delivering high-value, patient-centered care.
Early Diagnosis and Risk Stratification
One of the most notable changes in the 2025 guidelines is the emphasis on early recognition of disease. COPD is still underdiagnosed, often detected only after substantial lung function decline.
- At-risk populations: Smokers, former smokers, individuals with occupational exposures (e.g., dust, biomass fuels), and those with chronic cough or unexplained dyspnea are highlighted for earlier evaluation.
- Spirometry remains essential: The guidelines reaffirm spirometry as the gold standard for diagnosis, but now recommend its broader use in at-risk patients—even before significant symptom burden develops.
- Imaging refinements: Low-dose CT and advanced imaging are increasingly recognized for phenotyping patients, particularly those with discordant symptoms and spirometry results.
The goal is to identify COPD earlier, stage it more precisely, and intervene before irreversible decline.
Pharmacologic Therapy: A Personalized Approach
Pharmacologic management has shifted from a purely symptom/exacerbation model toward a phenotype- and biomarker-driven strategy.
- Initial therapy: For Group A patients, inhaled bronchodilator (short acting or long acting bronchodilator) may be enough. If available and affordable, a long acting bronchodilator is preferred unless the patient has very occasional breathlessness. For Group B patients, preference for dual therapy (LABA/LAMA) in those with significant symptom burden. If that is not feasible, either LAMA or LABA may be used and combination therapy is advised if not adequate control.
- Role of ICS: Inhaled corticosteroids (ICS) are now guided more clearly by blood eosinophil counts. Patients with eosinophils ≥300 cells/µL or frequent exacerbations benefit most from ICS-containing regimens.
- Triple therapy (ICS/LABA/LAMA): Stronger evidence supports triple therapy for patients with severe disease, high exacerbation risk, or persistent symptoms despite dual therapy.
- De-escalation: The guidelines also address stepping down therapy when risks outweigh benefits, particularly for ICS in patients with low eosinophils and recurrent pneumonia.
This precision-medicine approach reflects a more nuanced understanding of COPD pathophysiology.
Non-Pharmacologic Interventions
The 2025 guidelines place renewed focus on non-drug therapies that have proven survival and quality-of-life benefits:
- Pulmonary rehabilitation: Now recommended not only post-exacerbation but also for stable patients with functional limitations.
- Smoking cessation: Still the single most impactful intervention—guidelines call for intensified behavioral counseling, pharmacotherapy, and digital tools.
- Vaccinations: Expanded recommendations now include RSV vaccination for older adults and those with chronic lung disease, alongside influenza, pneumococcal, and COVID-19 vaccines.
- Lifestyle and nutrition: Attention to physical activity, weight optimization, and muscle preservation are emphasized as part of comprehensive care.
Exacerbation Prevention and Long-Term Follow-Up
Preventing exacerbations is considered equally important as symptom relief in the new guidelines. Exacerbations accelerate lung function decline, reduce quality of life, and increase mortality risk.
Key updates include:
- Closer follow-up: Post-exacerbation visits are recommended within 1 month, with ongoing reassessment of inhaler technique, adherence, and comorbidities.
- Digital health: Remote monitoring and digital inhaler sensors are now acknowledged as promising tools for detecting early decompensation.
- Adjunctive therapies: Consideration of chronic azithromycin, roflumilast, or mucolytics in select high-risk patients.
Comorbidities and Holistic Care
COPD rarely exists in isolation. The 2025 guidelines highlight systematic screening and management of common comorbidities:
- Cardiovascular disease (especially heart failure and coronary disease)
- Osteoporosis (from both systemic inflammation and corticosteroid use)
- Depression and anxiety
- Obstructive sleep apnea
- Diabetes and metabolic syndrome
The updated framework stresses integrated care models, encouraging collaboration across specialties to improve outcomes.
Implementation in Clinical Practice
While the science is clear, applying these recommendations in busy clinics can be challenging. The guidelines encourage:
- Team-based care: Involving nurses, pharmacists, and respiratory therapists in education and follow-up.
- Simplifying inhaler regimens: Preferring once-daily or combination devices to improve adherence.
- Point-of-care tools: Using visual aids, checklists, and decision-support algorithms.
Learn More at Our CME Conferences
At CME Travel Academy, we’ll be unpacking the 2025 COPD Guidelines in detail—not just the recommendations themselves, but also how to apply them in day-to-day practice.
Our sessions go beyond the slide deck. You’ll get:
- Evidence-based updates directly from the new guidelines
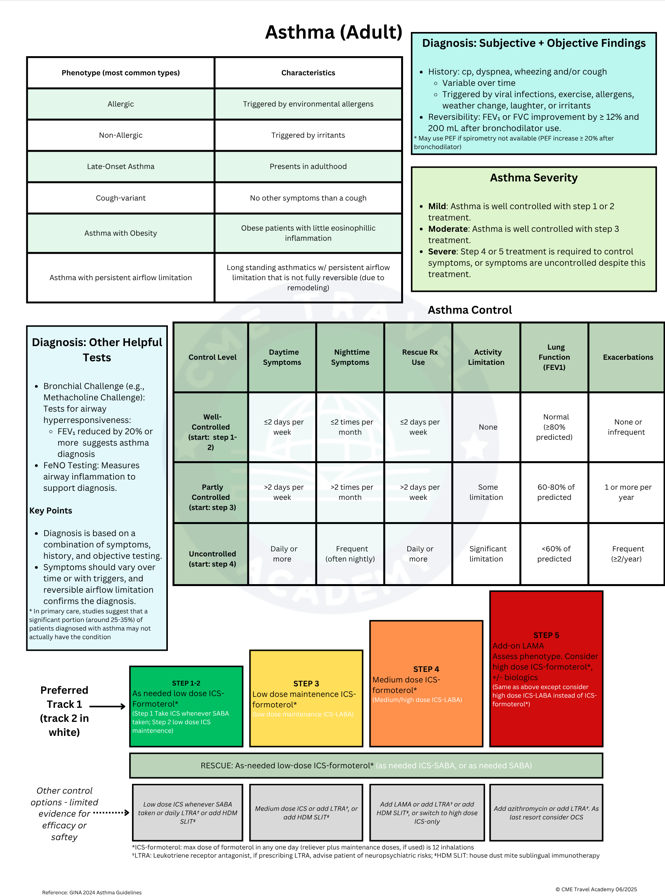
- One-page point-of-care references for quick use in clinic – sample
- 12 months of spaced repetition follow-up to keep knowledge fresh
- Engaging discussion of real-world cases and practical challenges
{kind=link}
You can join us at one of our upcoming destinations:
- Las Vegas, NV October 3-4, 2025 and February 20-21, 2026
- New Orleans, LA March 13-14, 2026
- San Diego, CA May 1-2, 2025 May 1-2, 2026
- Caribbean CME Cruise – COMING SOON
Bottom line: The 2025 COPD Guidelines mark a turning point toward earlier detection, personalized therapy, holistic care, and proactive exacerbation prevention. Staying current isn’t just about checking a CME box—it’s about changing the trajectory for patients living with COPD.